Sinus Floor Elevation and Bone Augmentation

Clinical Cases



Lateral Sinus Elevation with 20-year follow-up
Clinical challenge
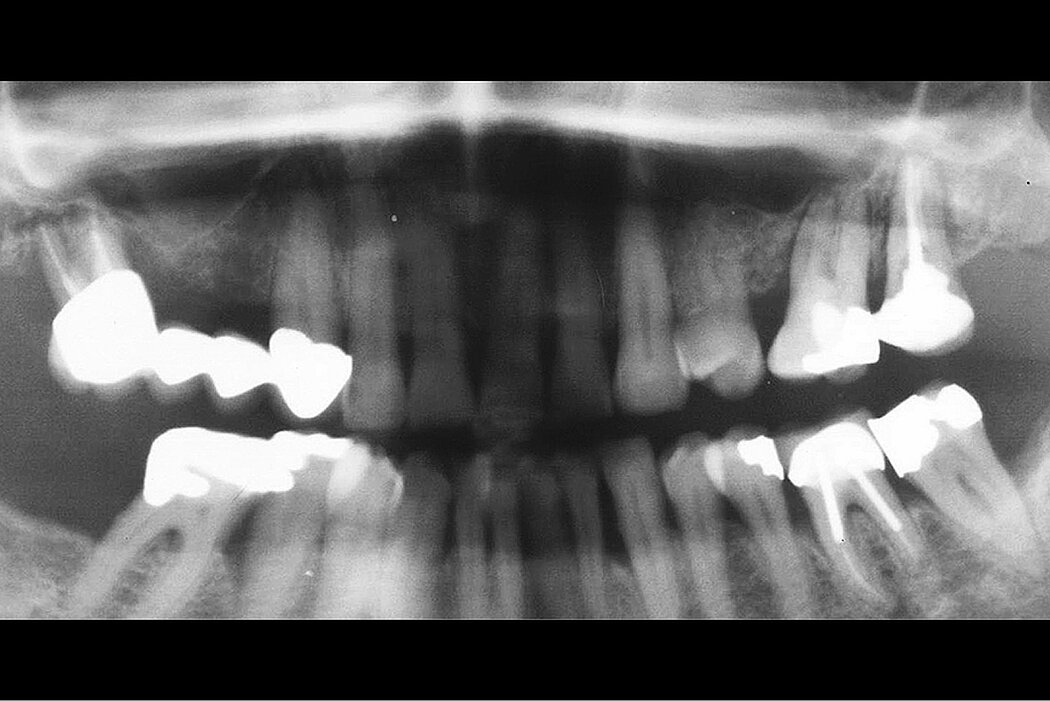
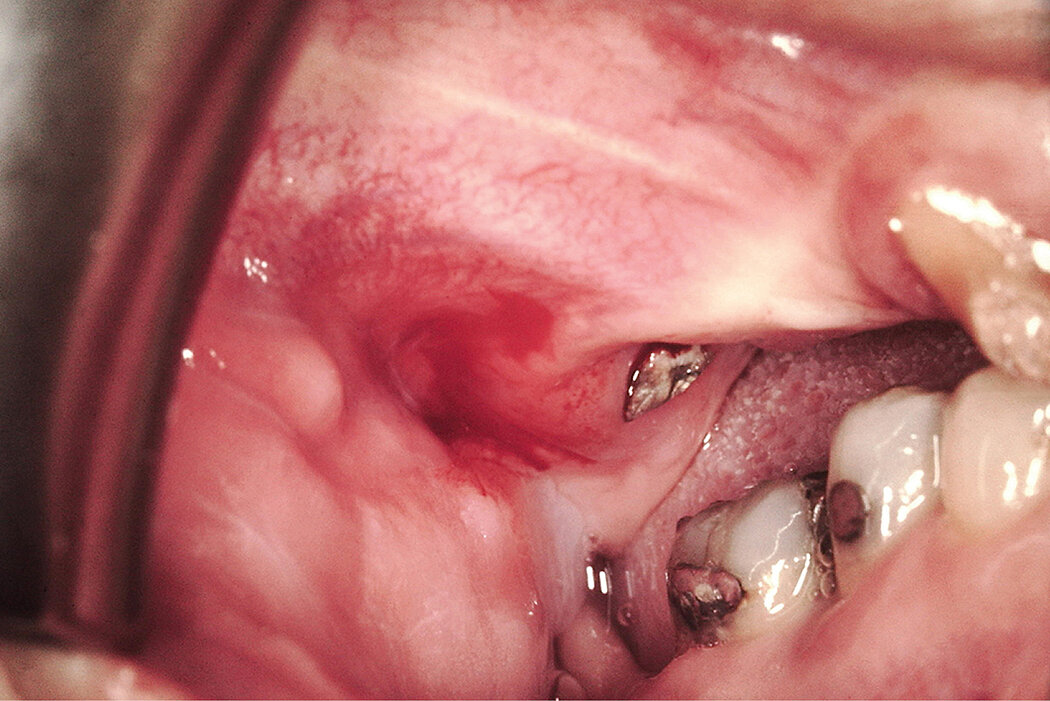
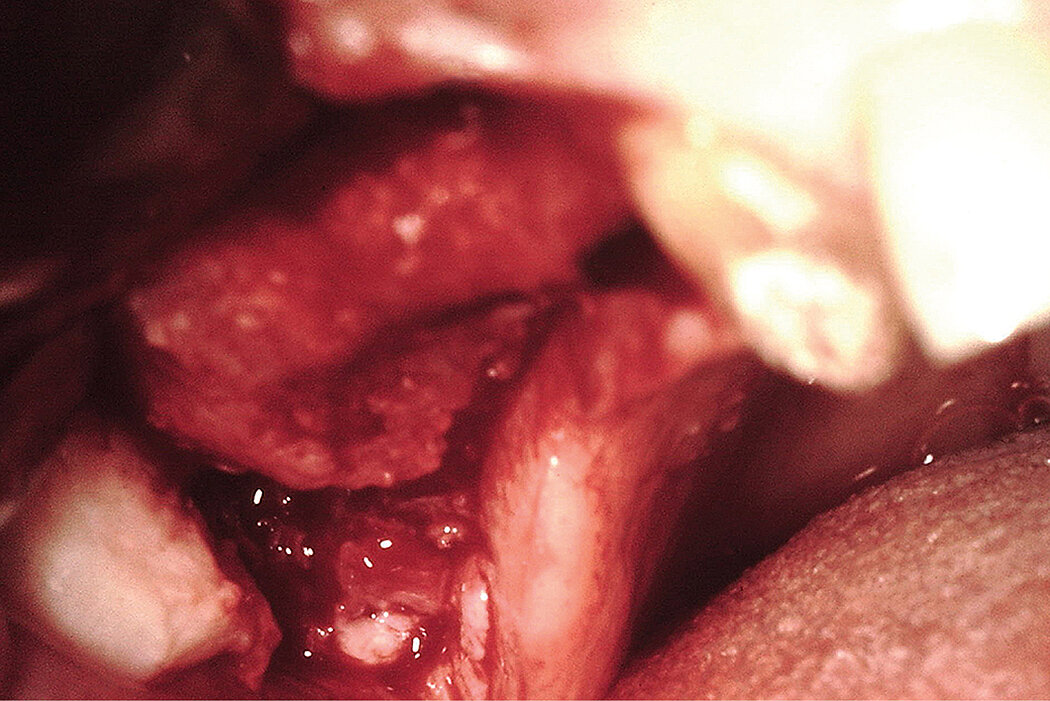
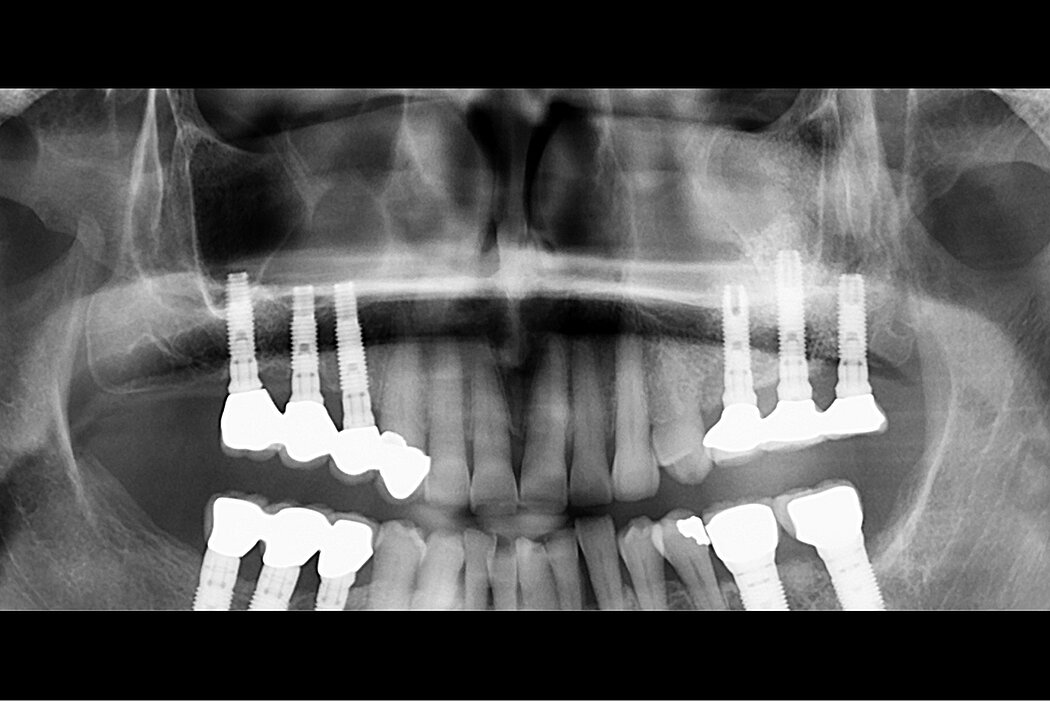
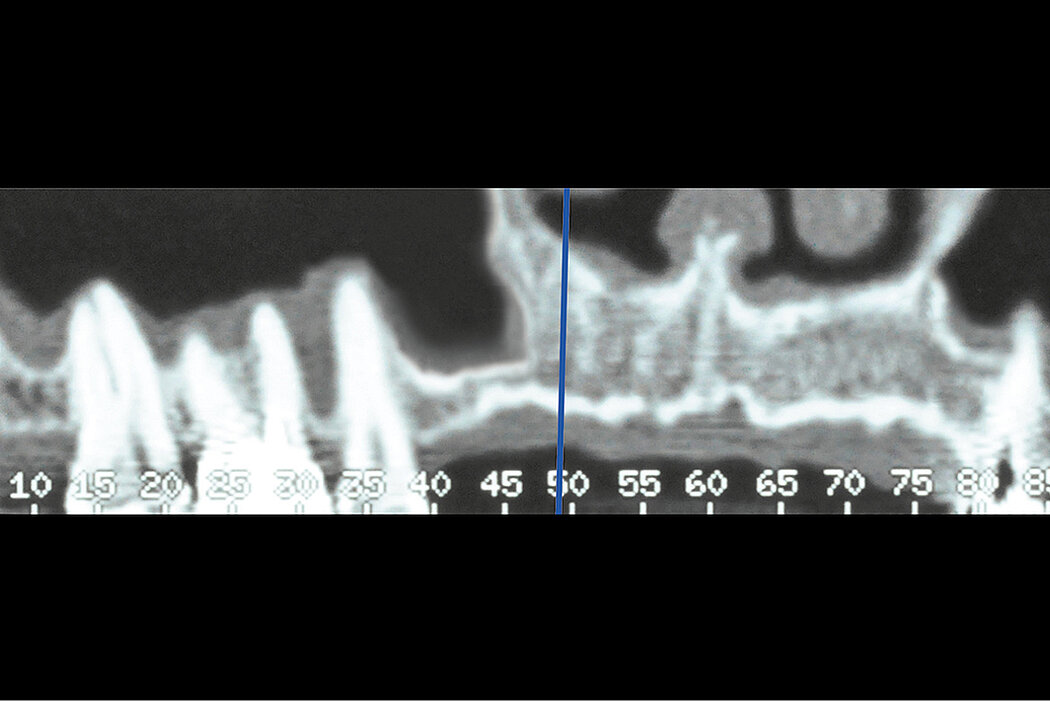
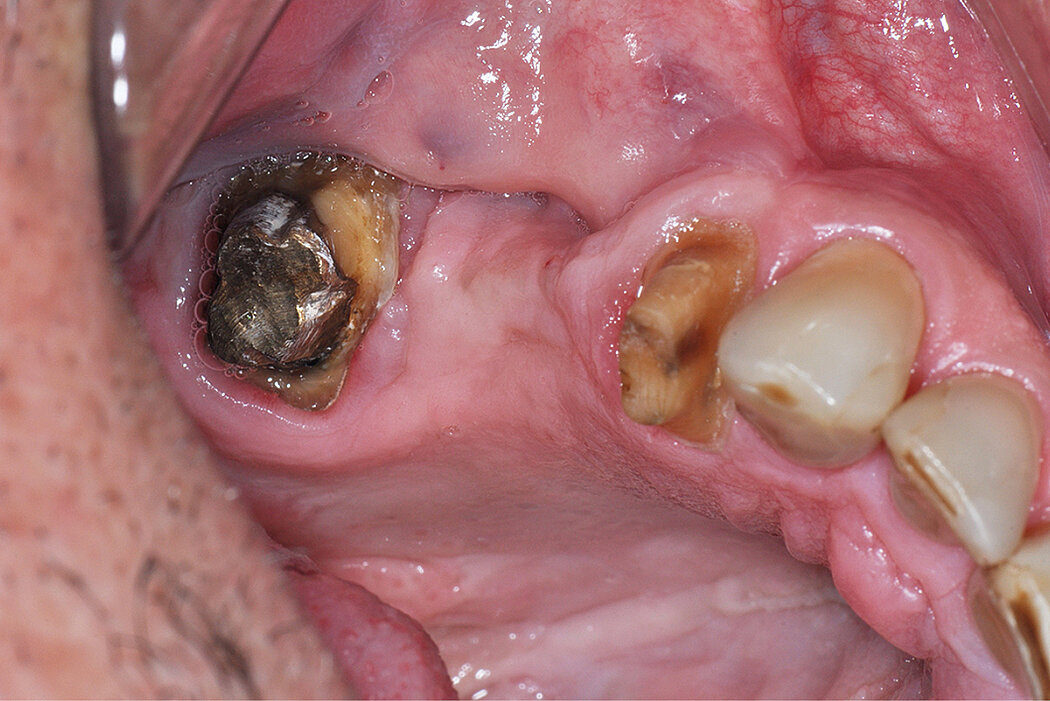
A 62-year-old female healthy patient was referred to the Schwartz-Arad surgical center for an extraction of the first right maxillary molar. This clinical case was performed in 1997 with a 20-year follow-up period. The region of interest is the right maxillary molar. In this region the 1st right maxillary molar was untreatable due to a perio-endo defect. The first and second right maxillary premolars were missing as well. The existing bridge included the right maxillary canine and the first molar. The available alveolar ridge was not sufficient for implant placement due to the pneumatization of the right maxillary sinus and the endo-perio-lesion of the tooth. The patient came for a treatment to obtain a fixed prosthetic restoration. The clinical challenge was to simultaneously reconstruct the ridge volume in the vertical dimension via a sinus augmentation procedure, and ridge preservation at the time of tooth extraction, for second stage implants placement.

Clinical outcome at a glance
Objectives
- Sinus floor elevation through a lateral window
- Bone augmentation of the maxillary sinus cavity prior to implant placement after 5 months
Conclusions
- Two-stage sinus floor elevation treatment
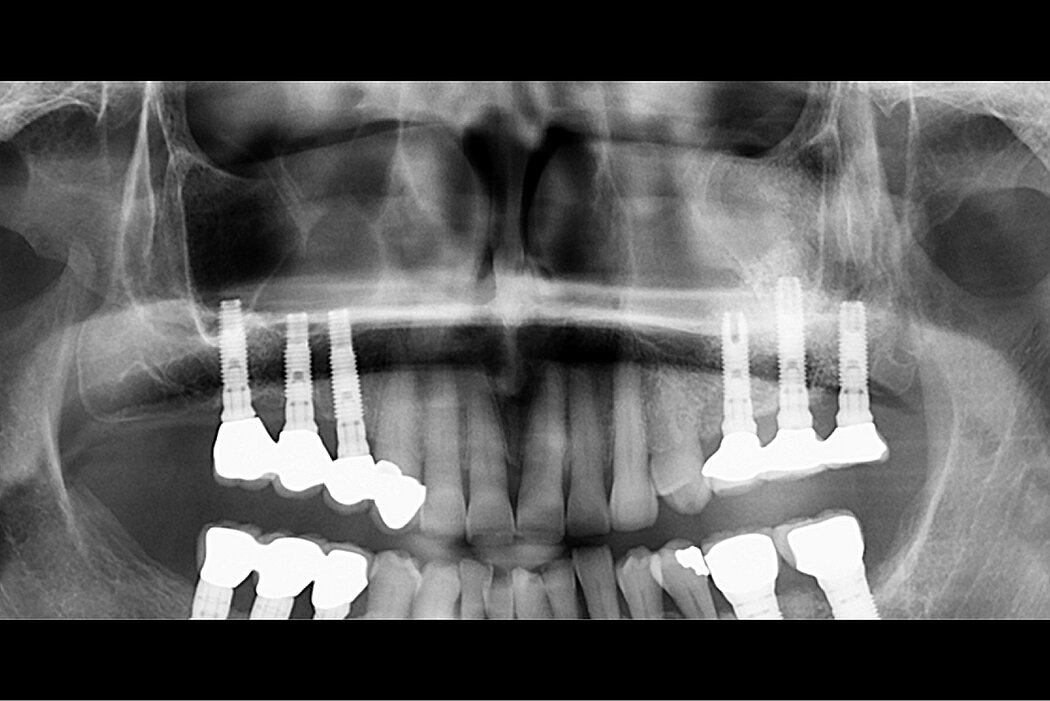
- Sinus floor elevation using Geistlich Bio-Oss® and Geistlich Bio-Gide® leads to long-term clinical success
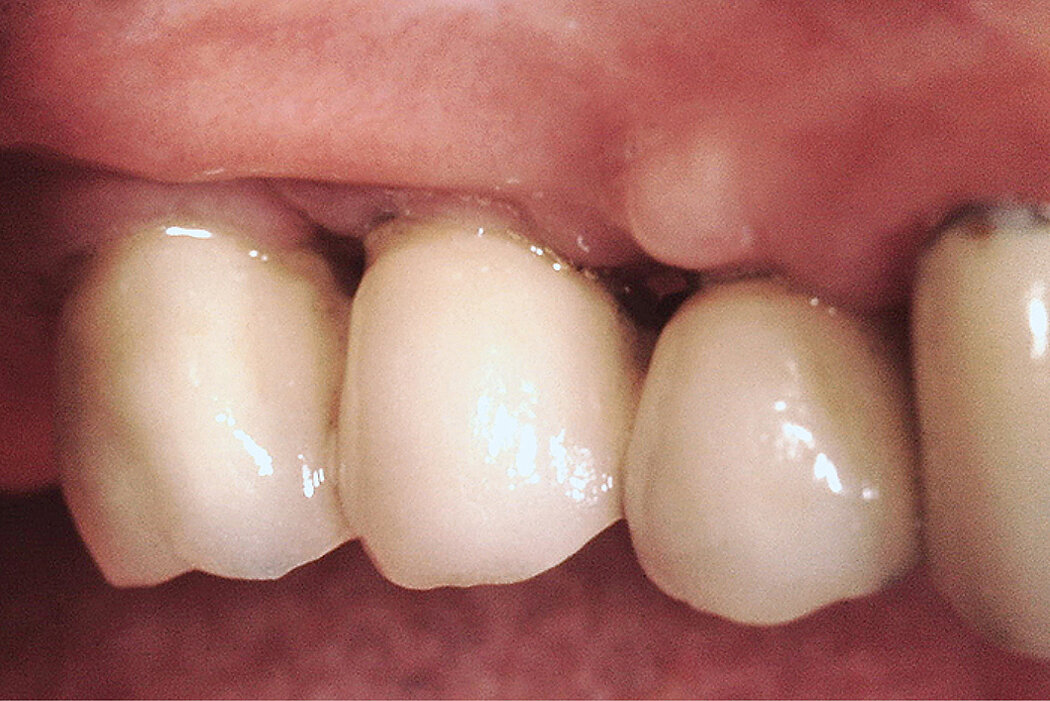
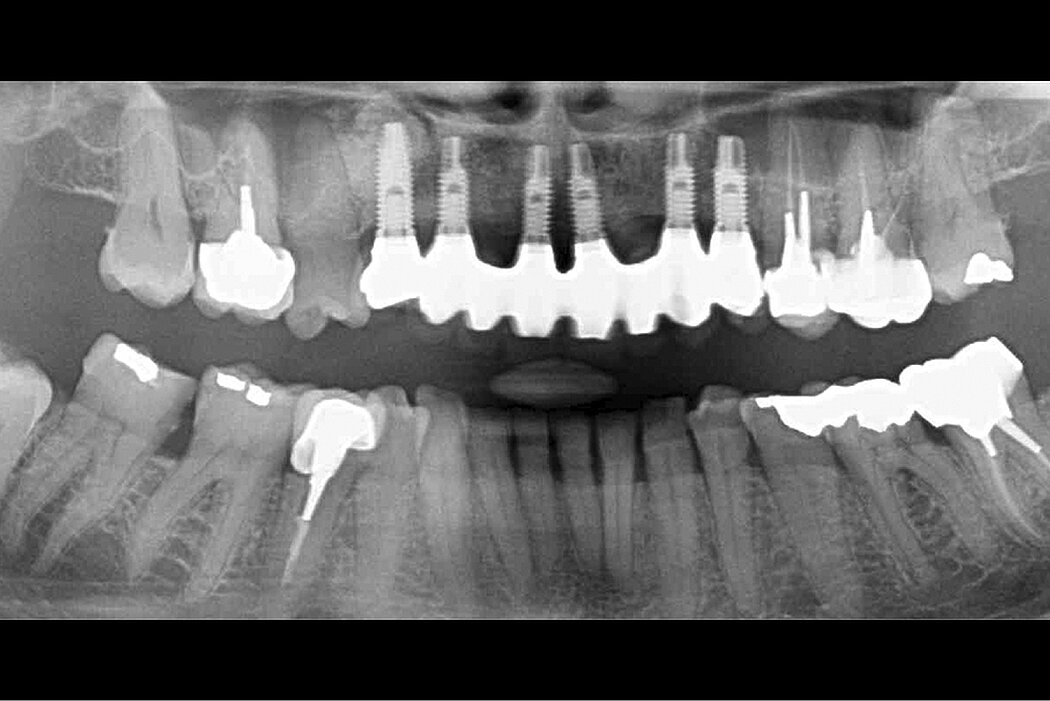
- Perfect prosthetic situation after 20-year follow-up

Aim / Approach
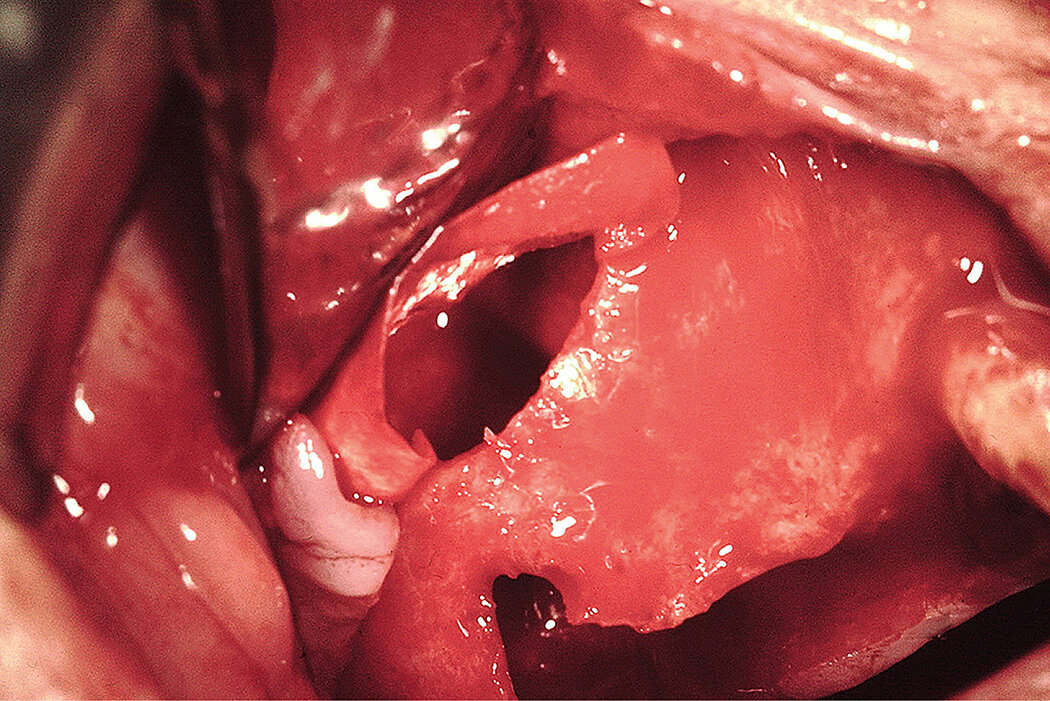
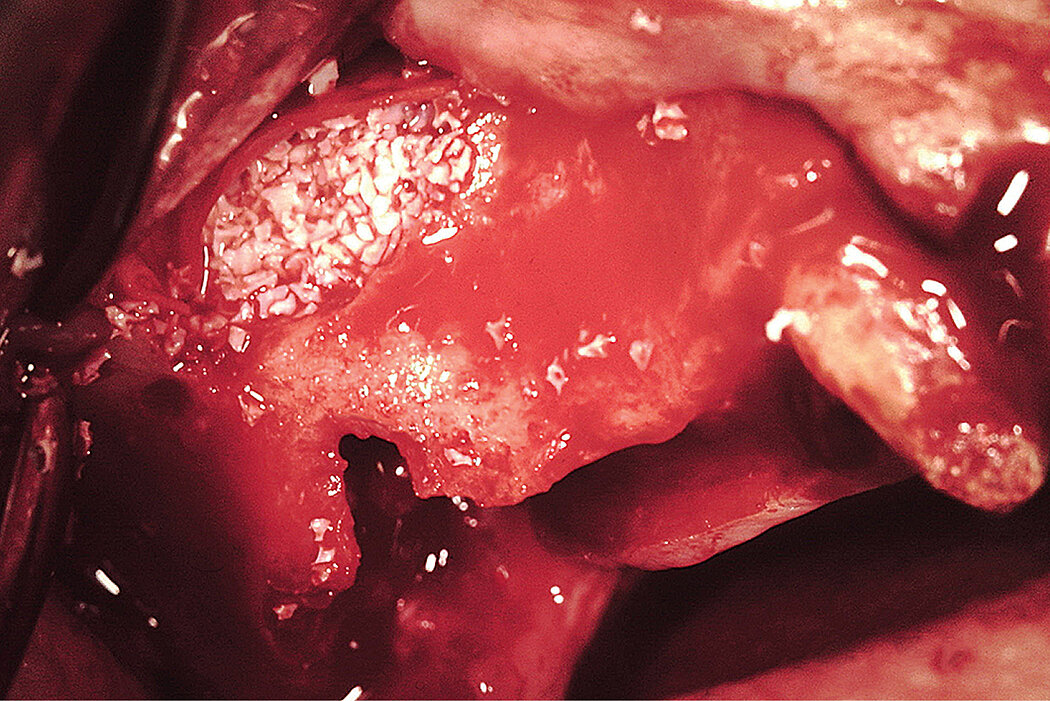
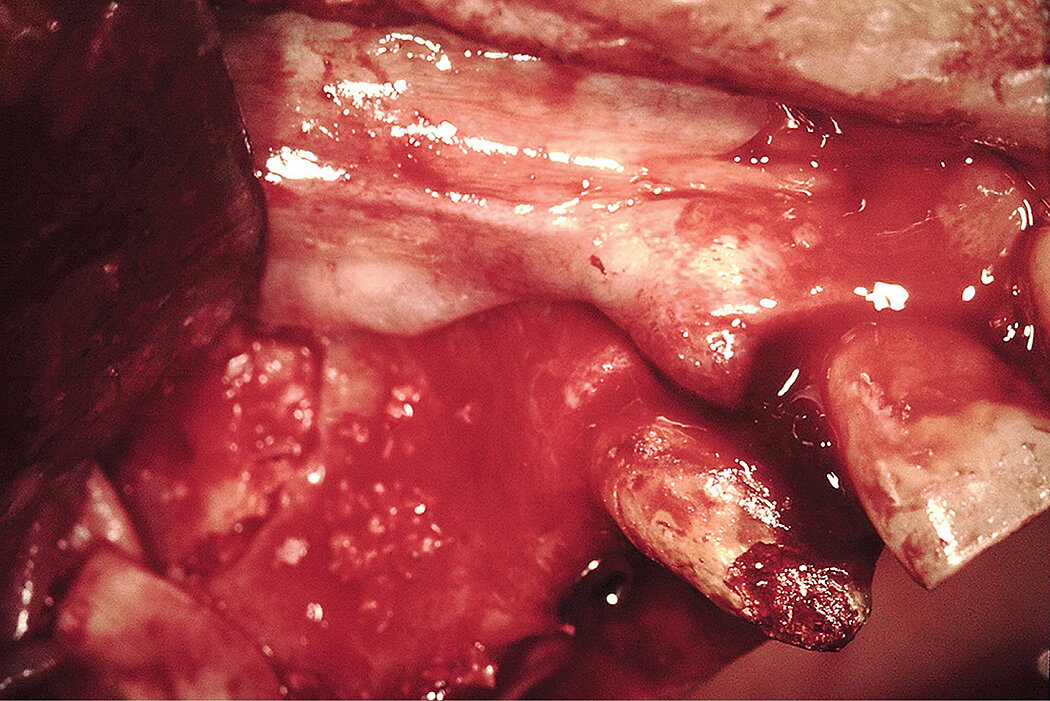
Sinus augmentation procedure via lateral window approach1
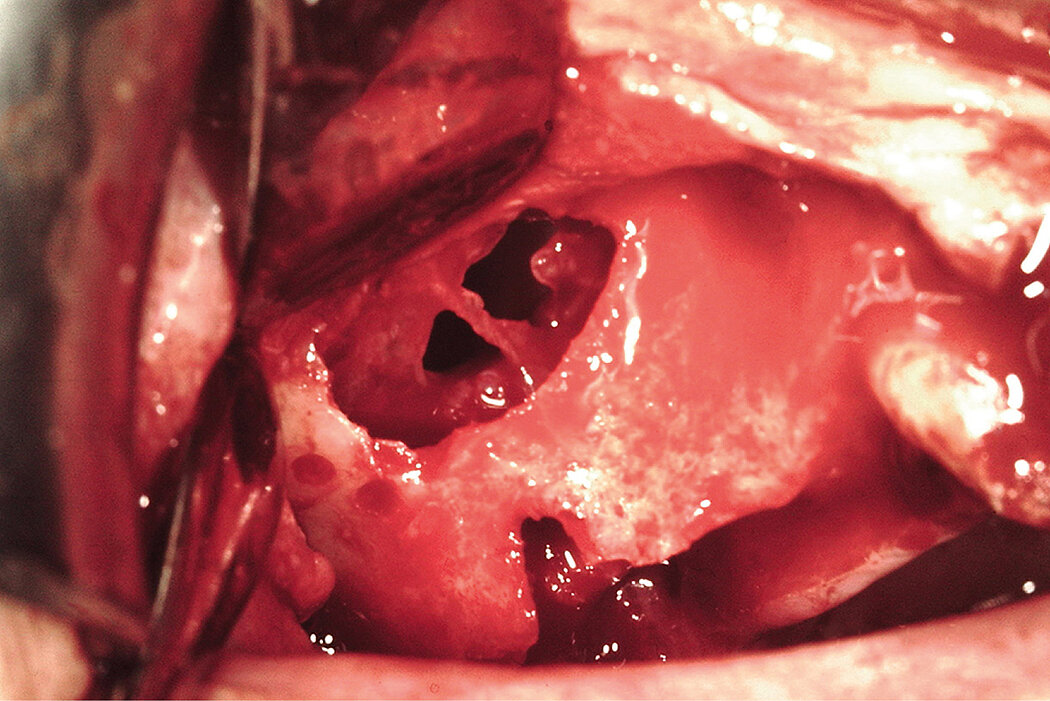
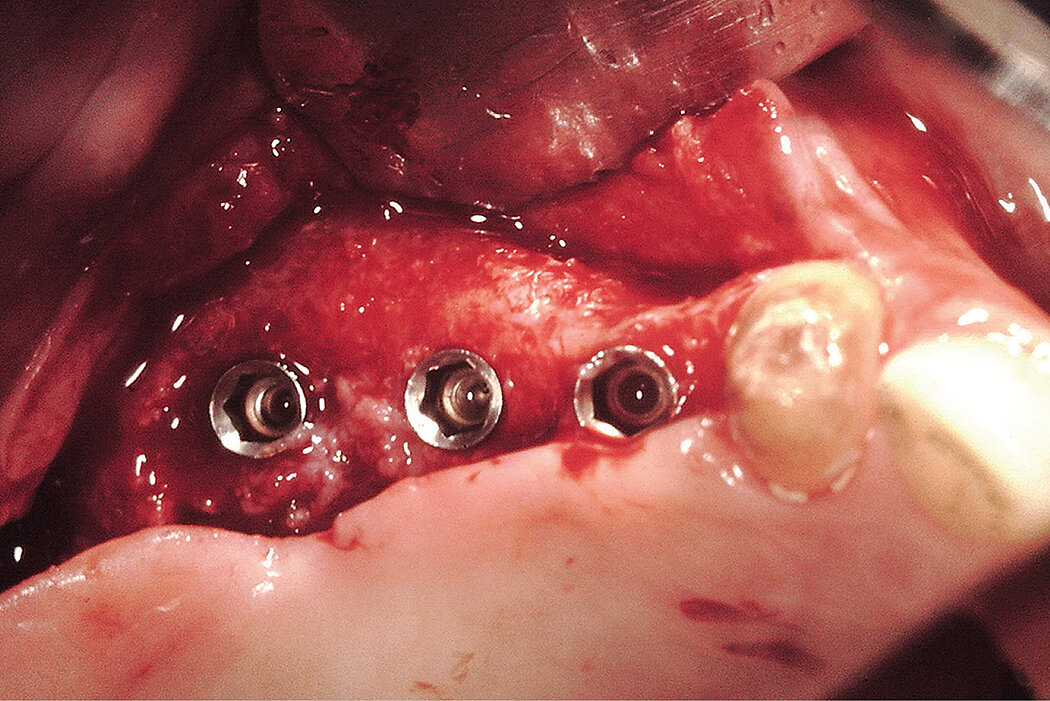
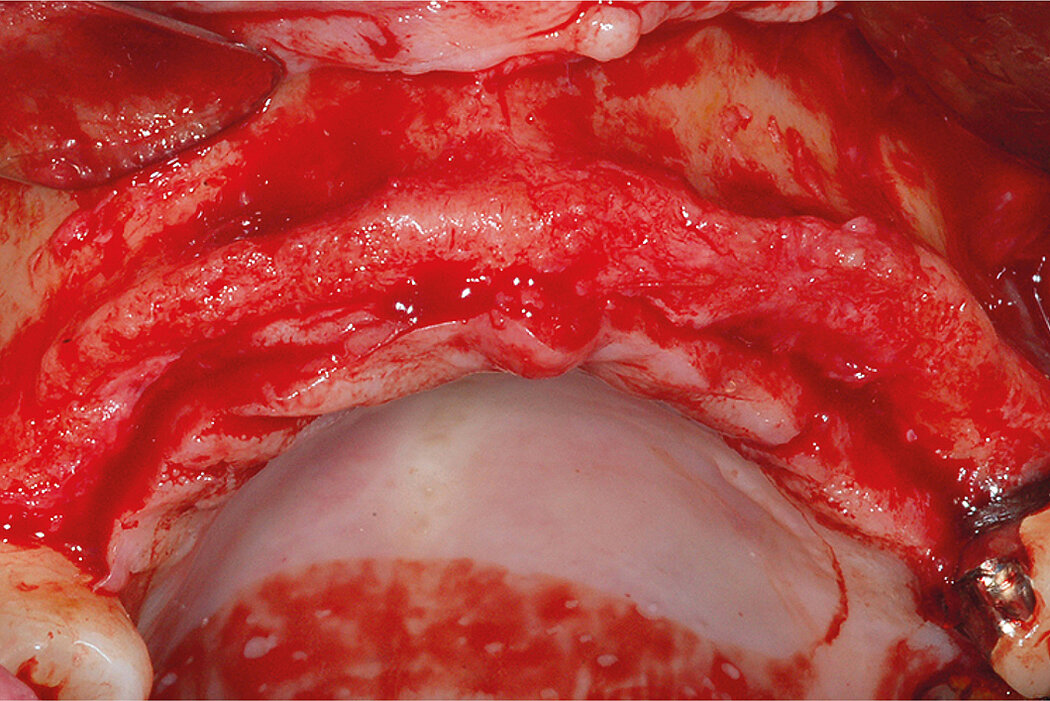
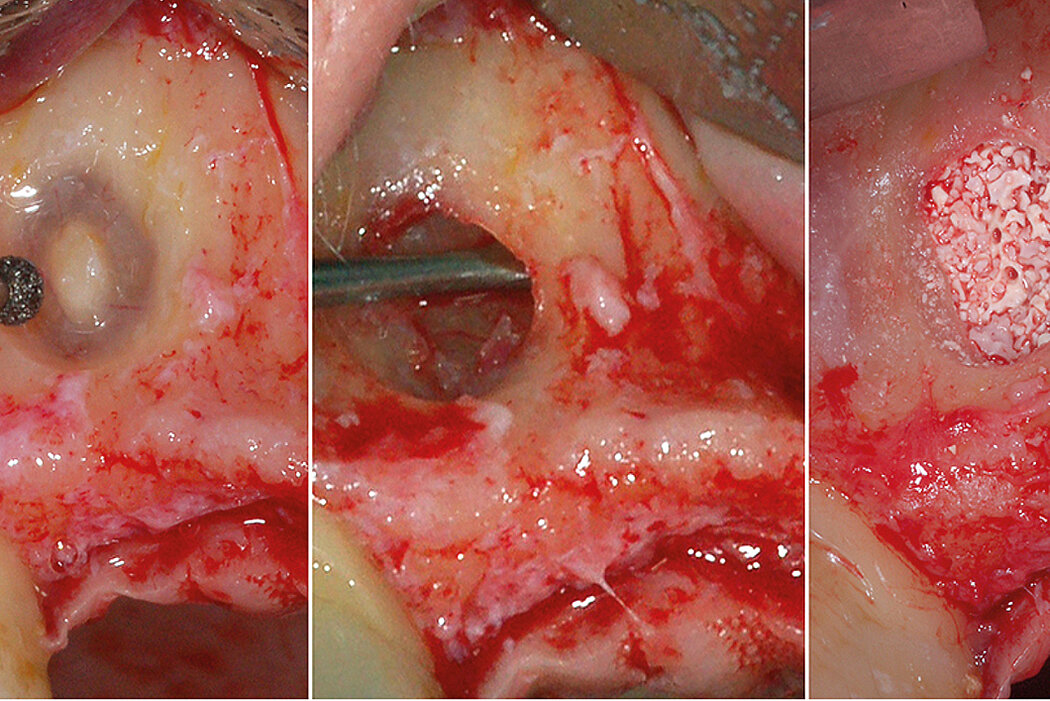
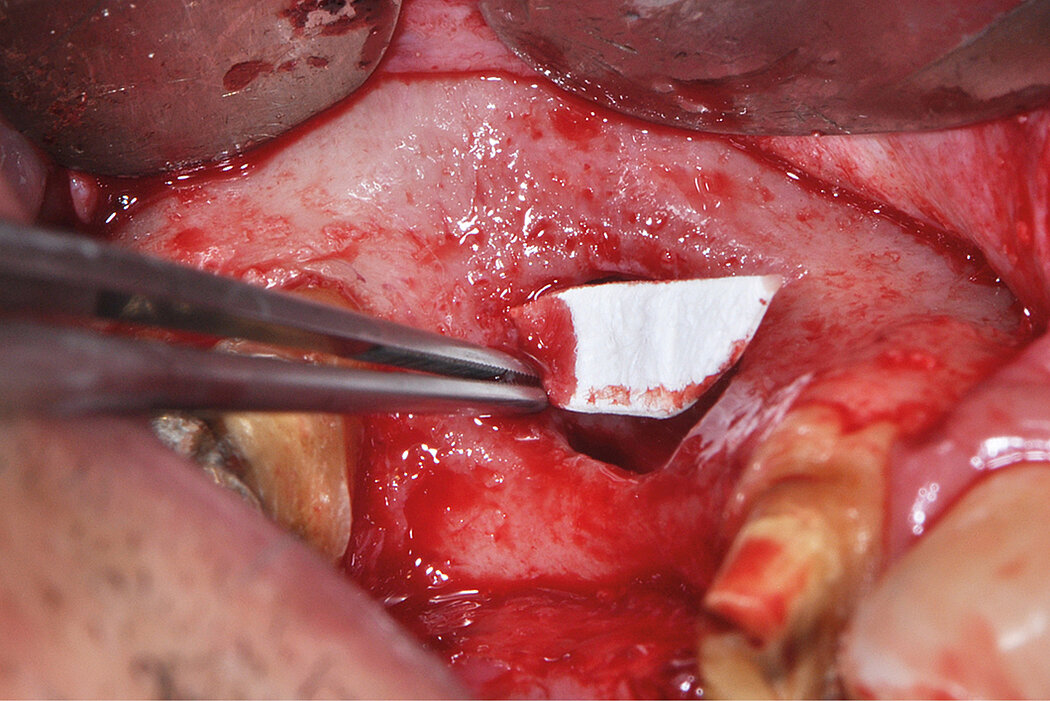
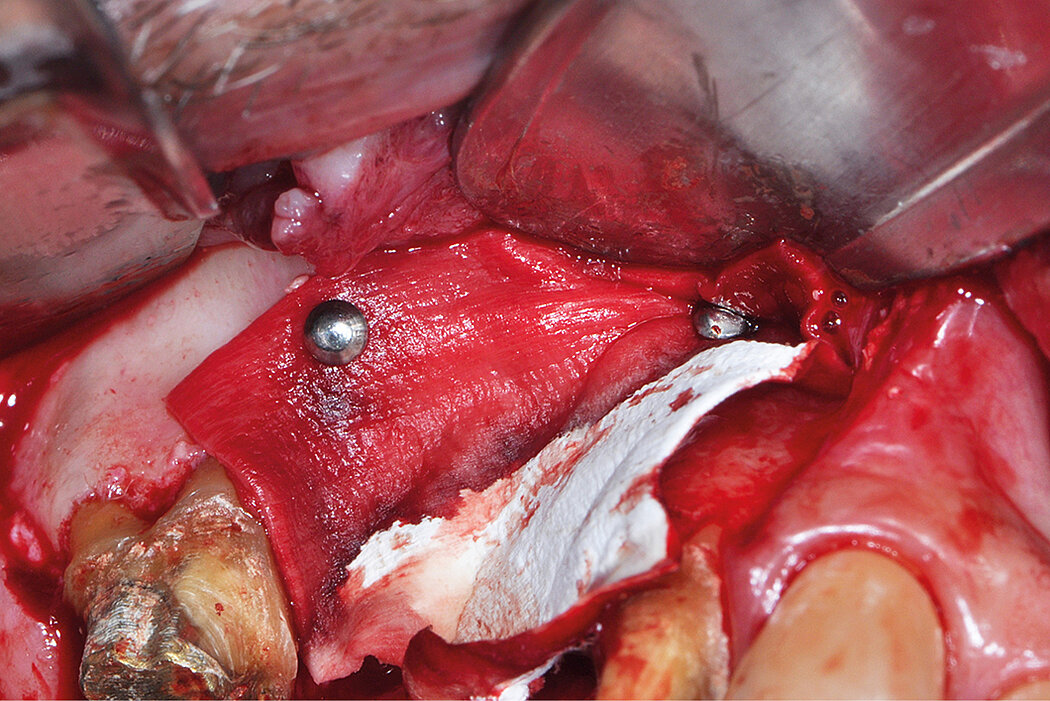
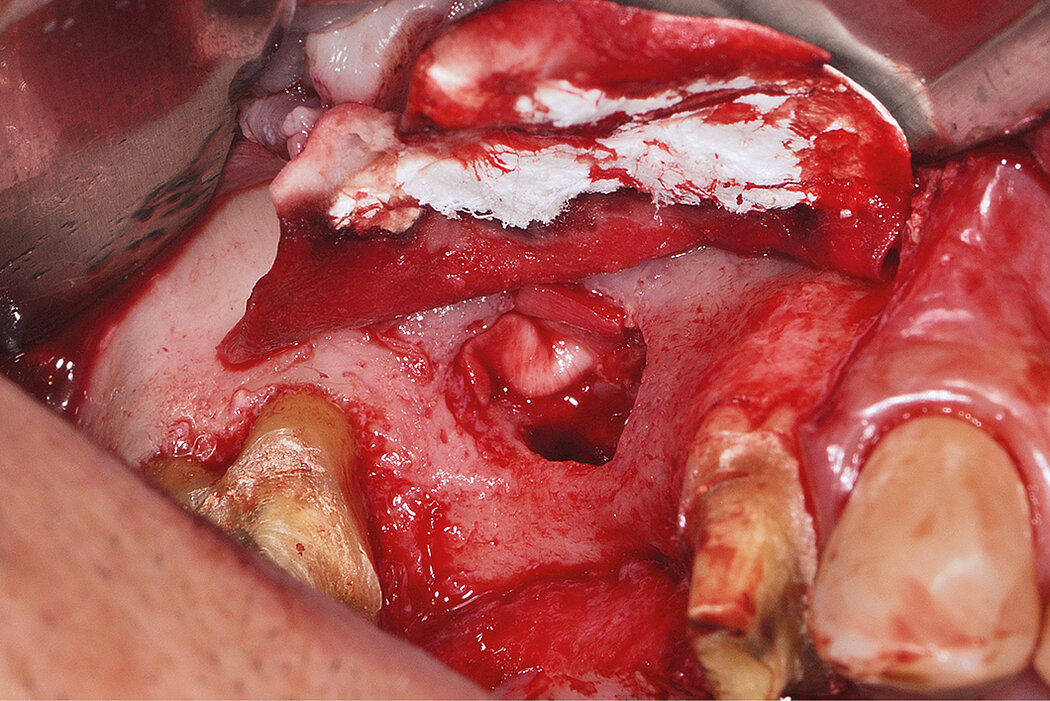
Prophylactic oral pre-medication of amoxicillin (1g) and dexamethasone (8mg) an hour before the procedure and a local application of 0.5% chlorhexidine for 2min. An incision was made on the alveolar crest and a vertical incision distal to the tuberosity was made to allow bone harvesting from this area to be mixed with the Geistlich Bio-Oss® . A window was cut through the lateral sinus wall cortex using a slow-speed round bone bur. At this point, the sinus membrane was carefully elevated from the sinus floor and medial sinus wall. Geistlich Bio-Gide® was used to repair the perforation. Since primary implant stability could not be attained, a delayed 2-stage implant placement was performed 5 months later. The maxillary sinus compartment was augmented with Geistlich Bio-Oss®. The fenestrated lateral wall of the maxillary sinus was covered with a Geistlich Bio-Gide® and the mucoperiosteal flap repositioned and sutured with a 3/0 Vicryl.
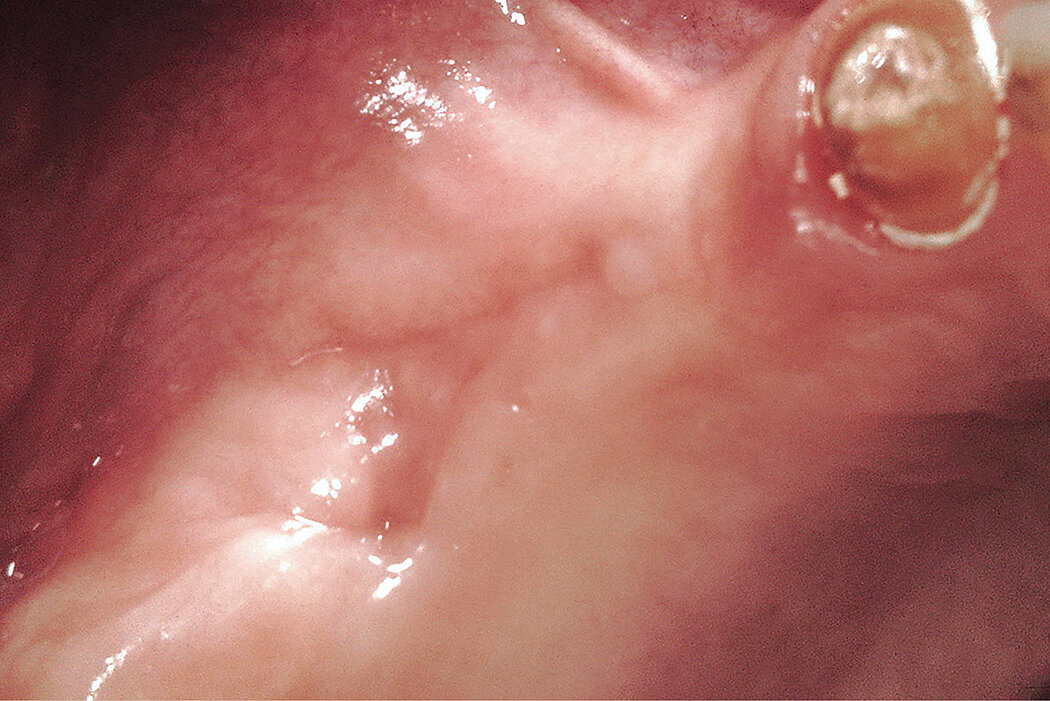
Conclusion
This case, with 20 year follow-up, is only one example of many patients with insufficient alveolar ridges, treated in the Schwartz-Arad surgical center with Geistlich Bio-Oss®. Bone augmentation using Geistlich Bio-Oss® and Geistlich Bio-Gide® for the sinus augmentation procedure is a predictable treatment approach for the long run. Furthermore, sinus membrane perforation did not influence implant success negatively when corrected with Geistlich Bio-Gide®.
References:
- Schwartz-Arad D et al., 2004. J Periodontol. Apr;75(4):511-6 (Clinical study).
Combination with 3D via F. Khoury’s technique
Clinical challenge
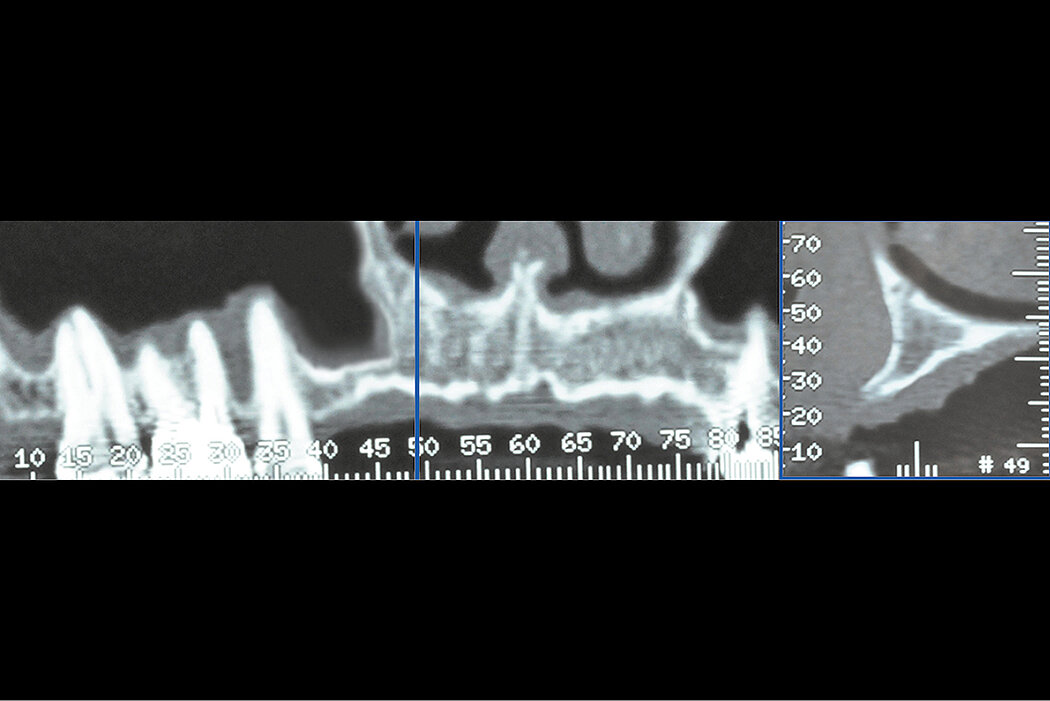
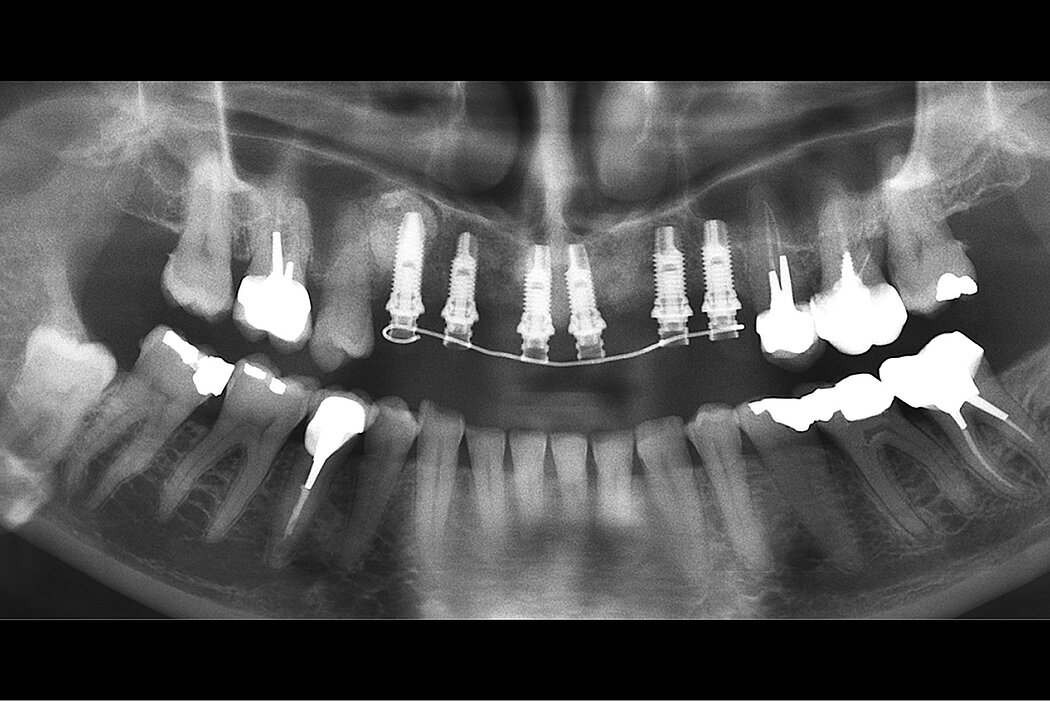
A pneumatized sinus cavity was localized in the area of the anteriormaxilla. Due to the atrophic alveolar crest it was impossible to place the implant in a correct position to achieve an appropriate esthetic rehabilitation.


Clinical outcome at a glance
Objectives
- Later sinus floor elevation in combination with bone regeneration with 3D using F. Khoury’s technique
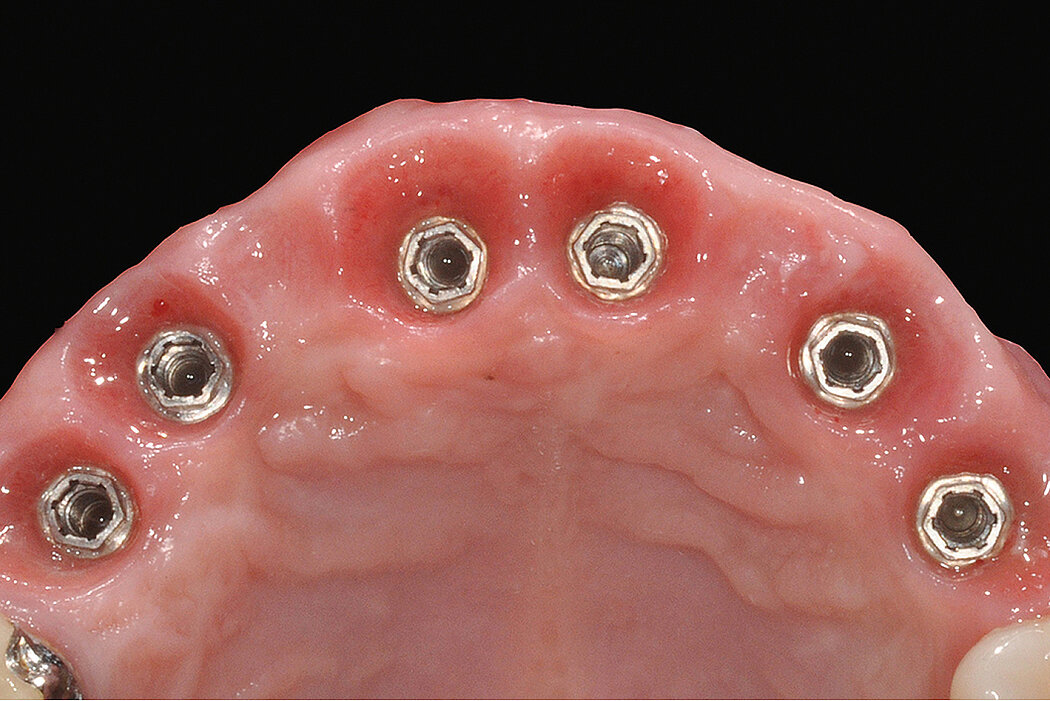
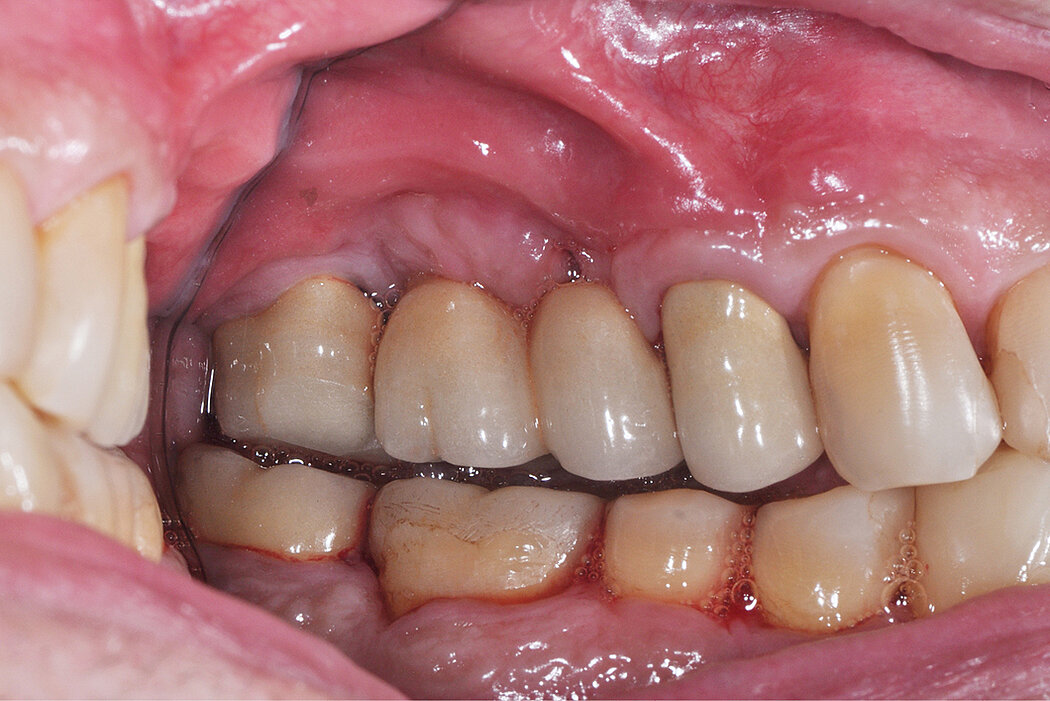
- Fixed prosthetic restoration in the upper and anterior area
Conclusions
- Two-stage sinus floor elevation treatment.
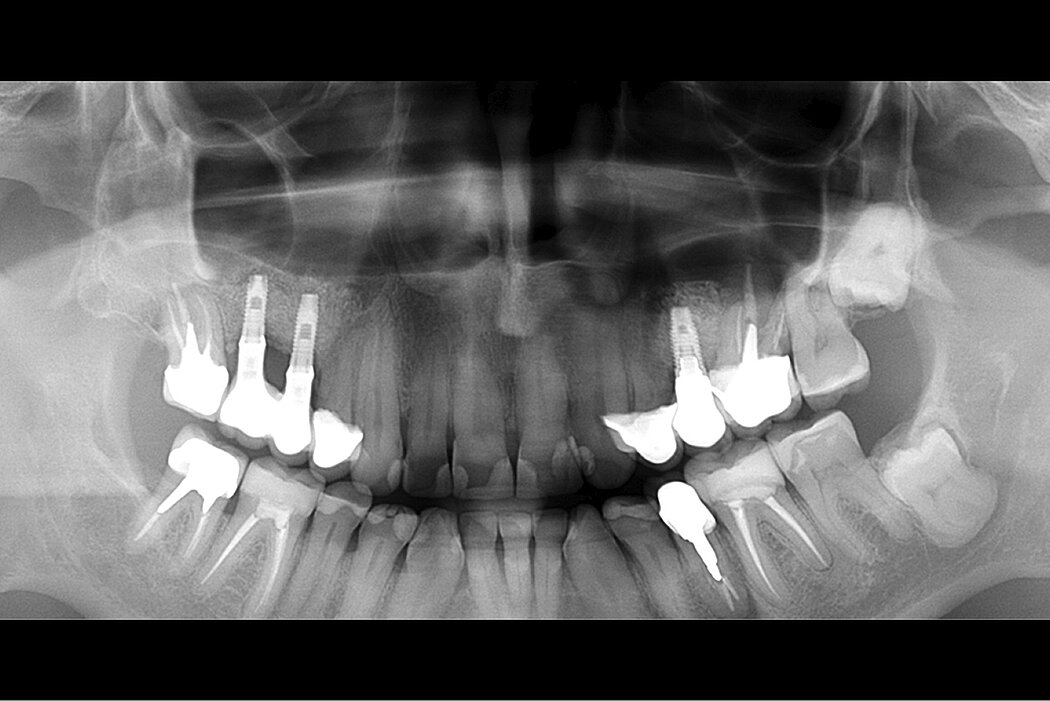
- Sinus floor elevation using Geistlich Bio-Oss® maintains long-term stability of the augmented bone volume
- Using Geistlich Bio-Oss® particles in combination with autologous bone chips limits the resorption rate of the augmented site

Aim / Approach
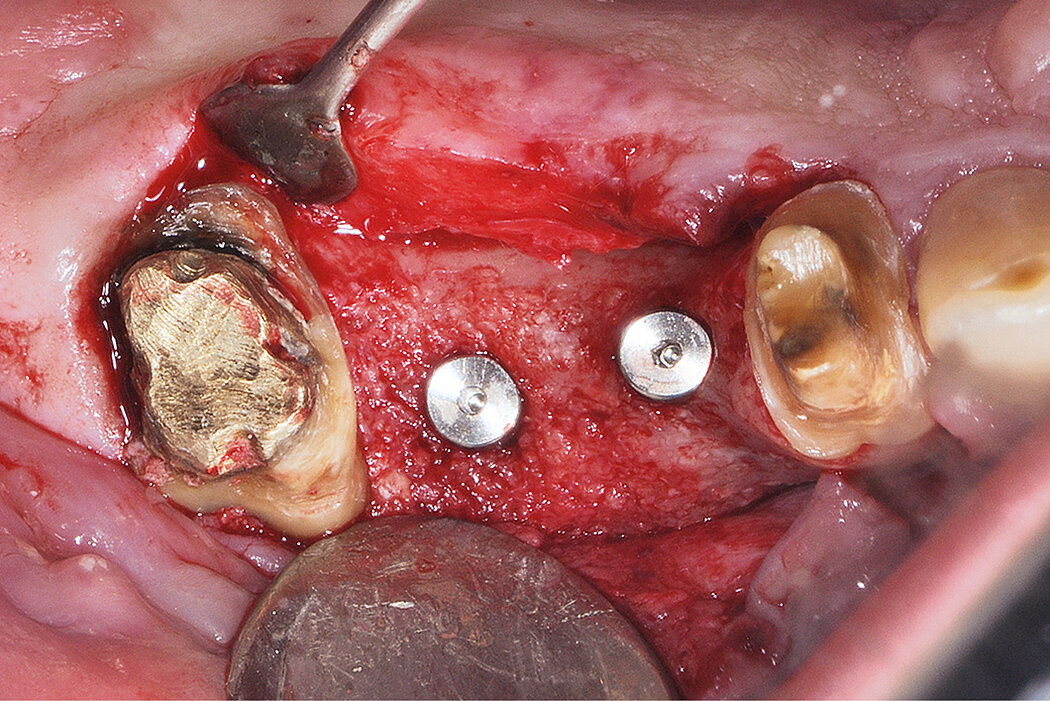
Lateral sinus floor elevation with Geistlich Bio-Oss® was performed in the area of the right canine/premolar. In this case the minimal invasivelateral window approach allows a better blood supply in the reconstructed region.
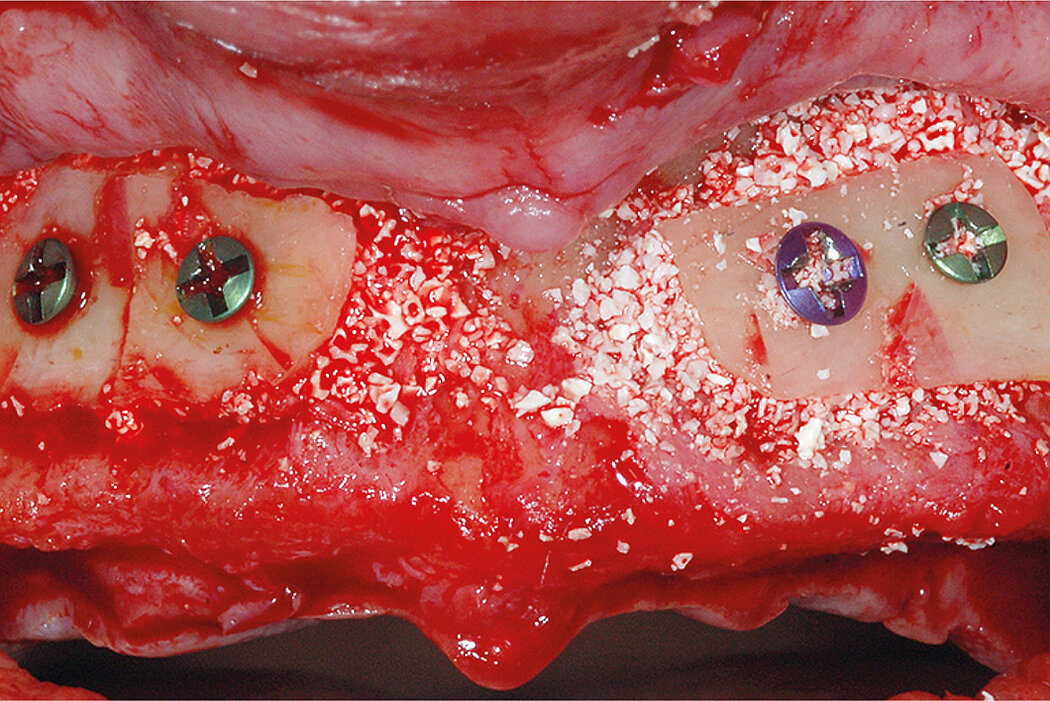
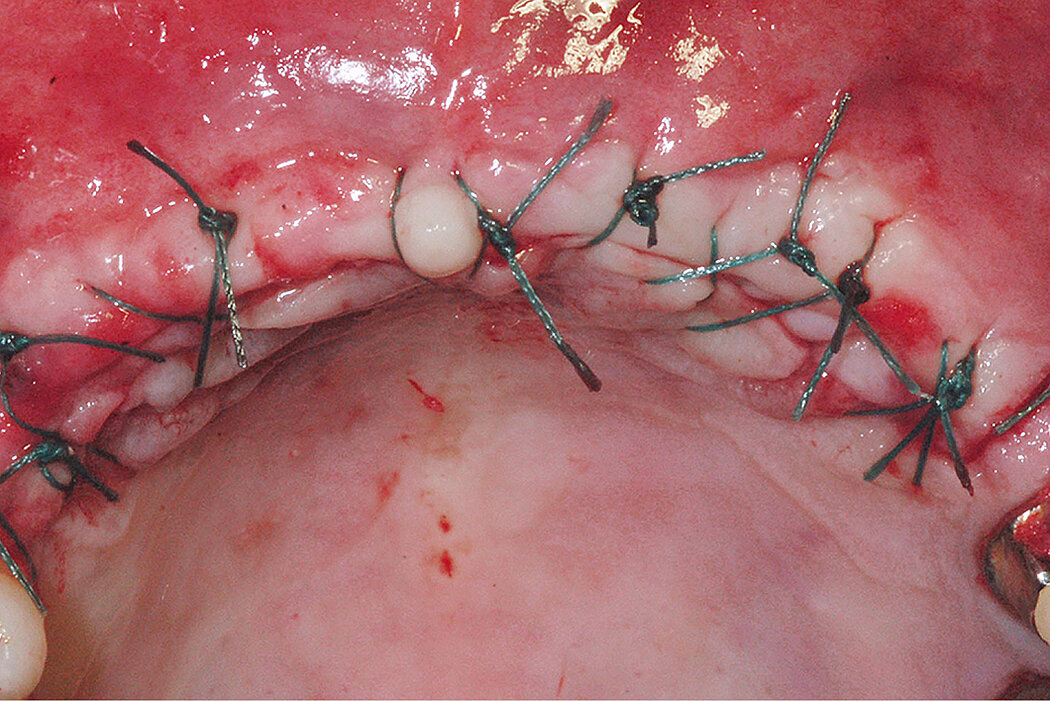
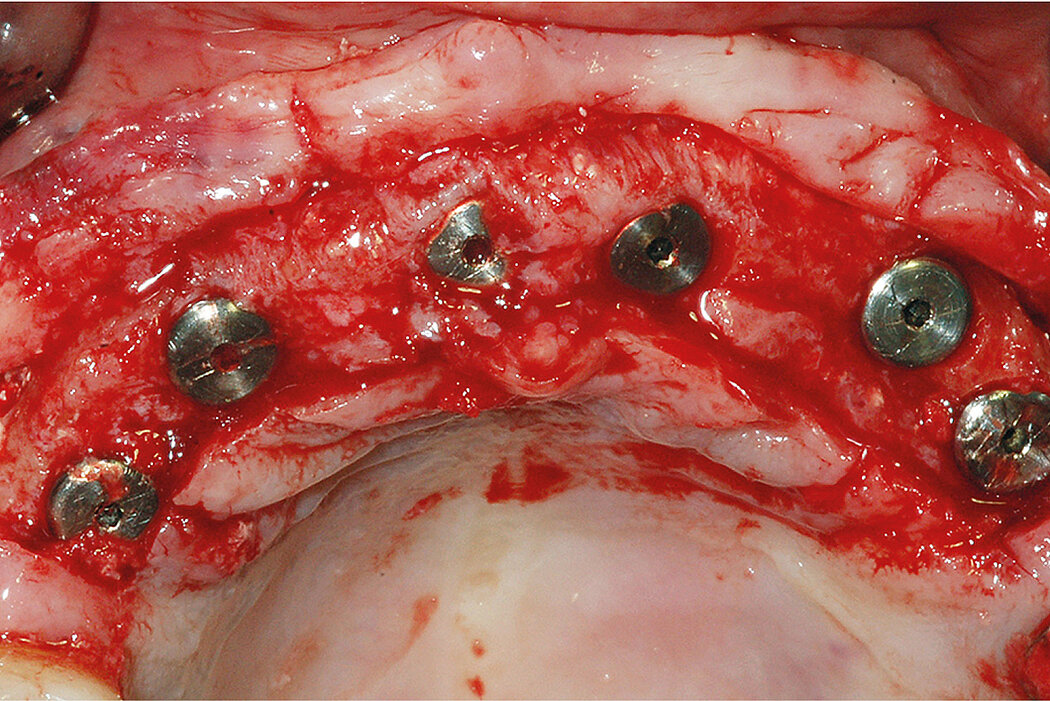
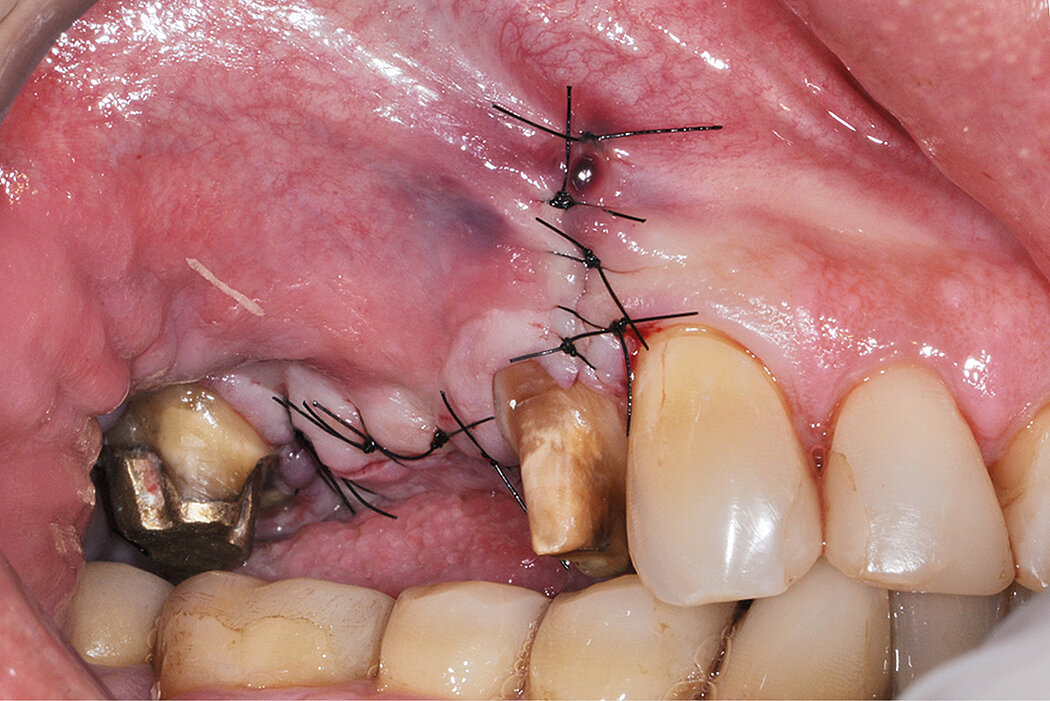
Following the sinus floor elevation abone reconstruction of the alveolar crest was performed with 3D using F. Khoury's technique. The bone block was harvested from the ramus. After preparation of the two blocks each were fixed with a screw in the upper frontal area. The residual spaces between and around the blocks were filled with a mix of Geistlich Bio-Oss® particles and autogenous bone chips.
Conclusion
Grafting with Geistlich Bio-Oss® particles in the sinus cavity maintains the long-term stability of the regenerated bone volume. It provides the patient a comfortable and predictable solution.
Reconstructing the alveolar crest with 3D via F. Khoury's technique in combination with the use of Geistlich Bio-Oss® minimizes the volume/size of the harvested bone block. Due to the slow resorption rate of Geistlich Bio-Oss® particles the bone volume is maintained and therefore the aesthetic result.
Reference:
- Hürzeler MB1, Weng D, 1999. Int J Periodontics Restorative Dent. Jun;19(3):279-87 (Clinical study).
Combination with guided bone regeneration
Clinical challenge
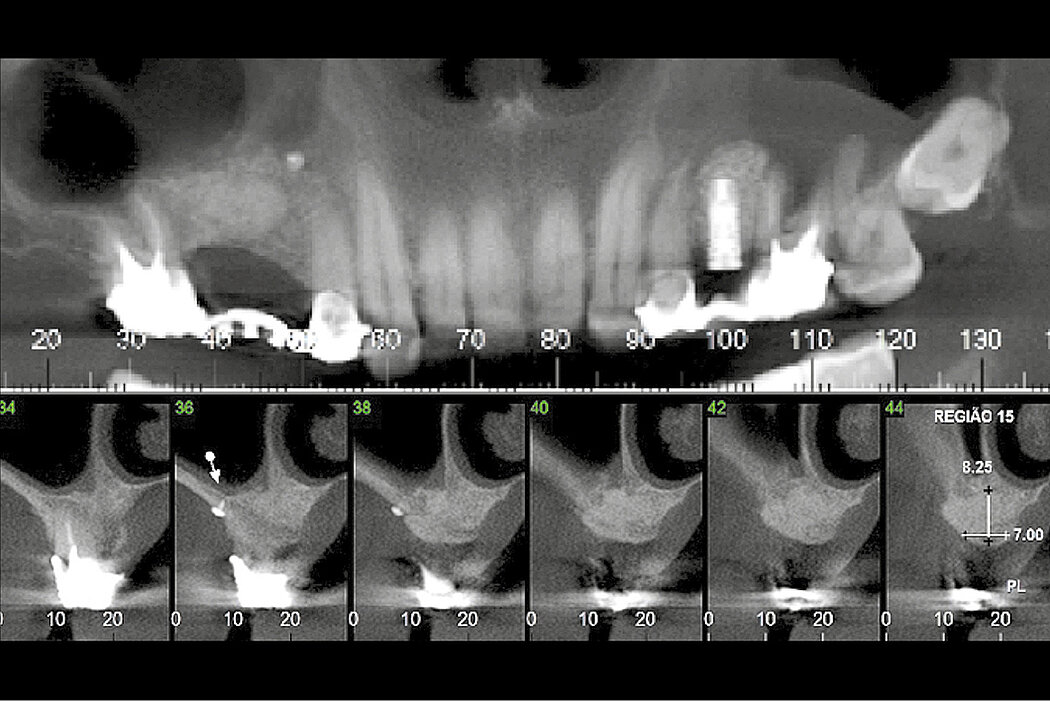
A difficult case of oral rehabilitation with a particular challenge at regions 15 and 16. The patient had a car accident some years before and was hit in this area. It resulted in an anatomical change to the sinus with partial loss of buccal sinus wall and scar tissue inside part of the sinus.
Clinical outcome at a glance
Objectives
- Challenging due to anatomic variations caused by previous car accident
- Sinus floor elevation with lateral window approach in combination with a guided bone regeneration
- Implant placement at 10 months after bone augmentation
Conclusions
- Two-stage sinus floor elevation treatment
- A sinus floor elevation in combination with a guided bone regeneration using Geistlich Bio-Oss® and Geistlich Bio-Gide® leads to stable bone volume for implant placement
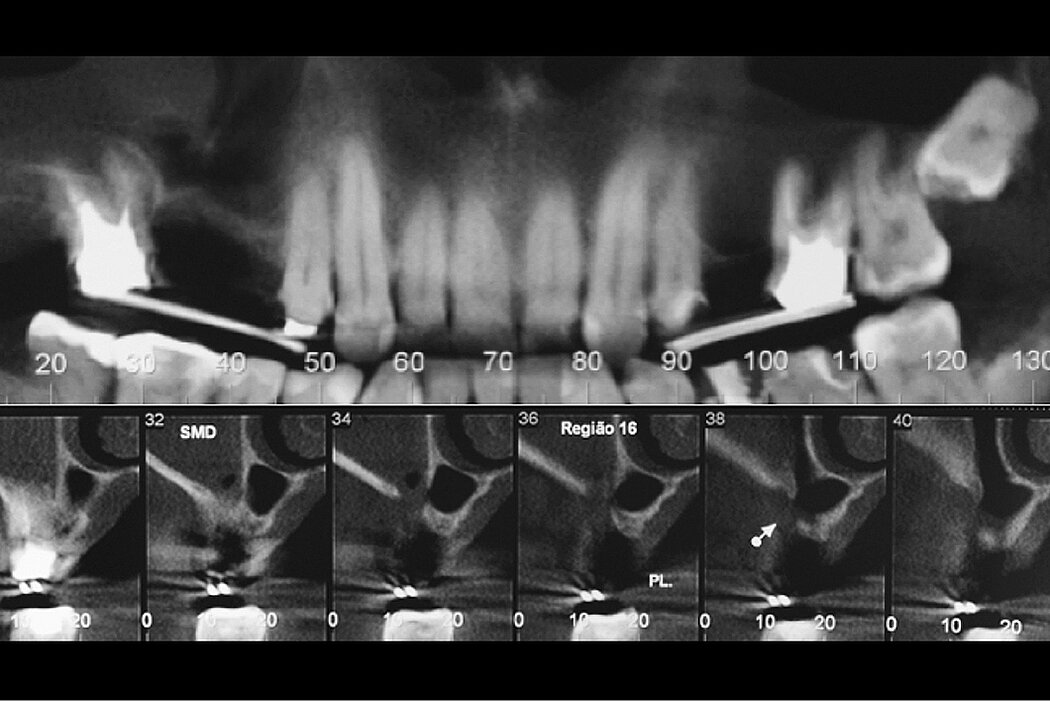
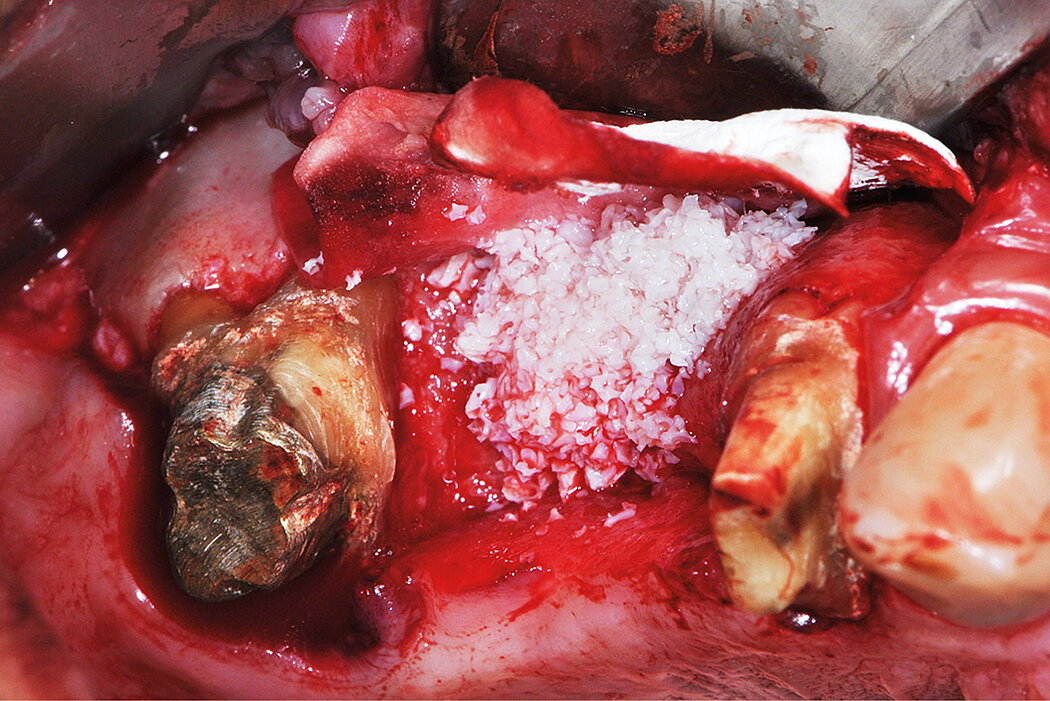
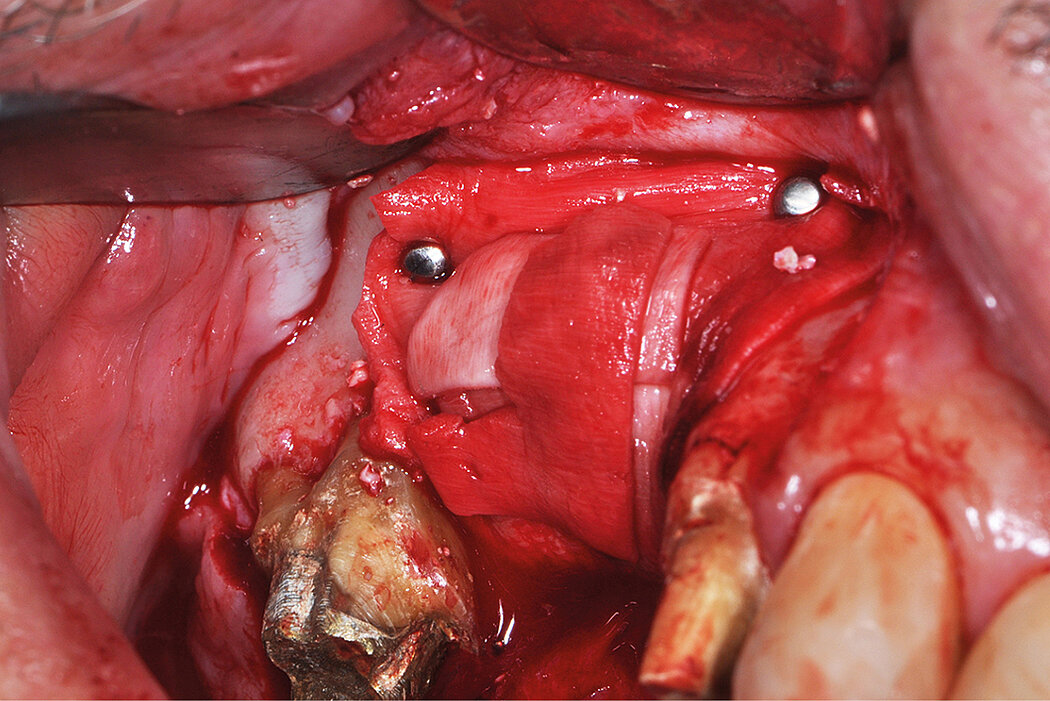
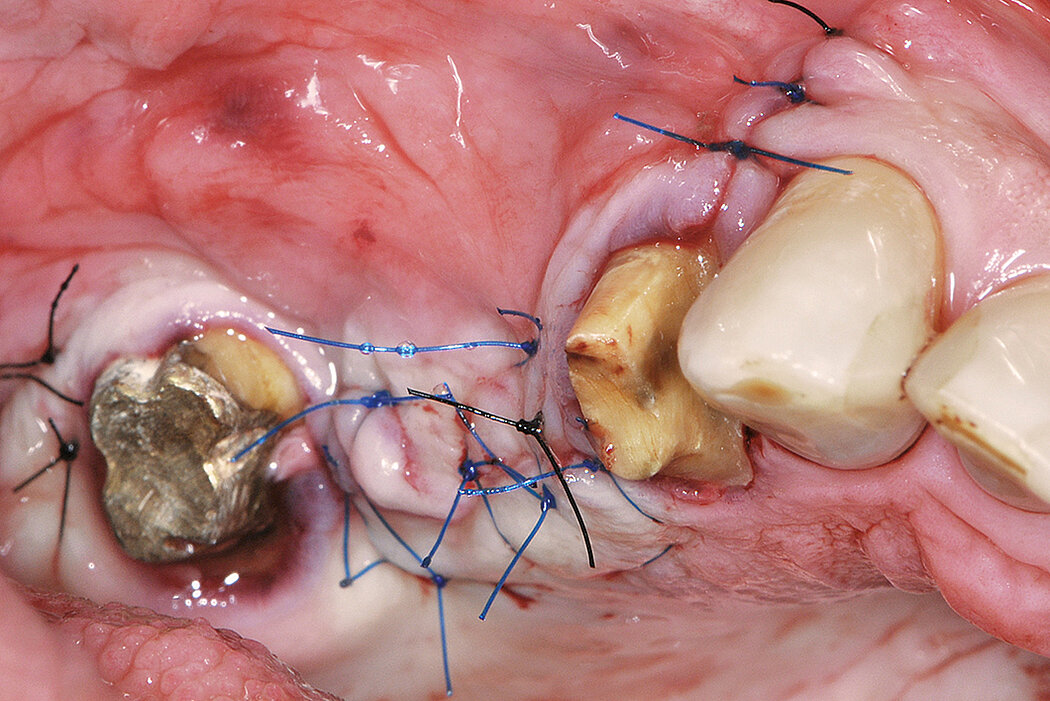
Aim / Approach
During flap reflection, the scar tissue was dissected and part of it removed. After this step, a Geistlich Bio-Gide® membrane was placed to isolate the fibrotic tissue present in the superior part of the sinus. Then the sinus membrane was elevated in the medial region of the sinus. The sinus cavity was filled with Geistlich Bio-Oss® which was also used to regenerate the ridge deficiency. Geistlich Bio-Gide® was stabilized buccally with bone tacks and packed in the palate.
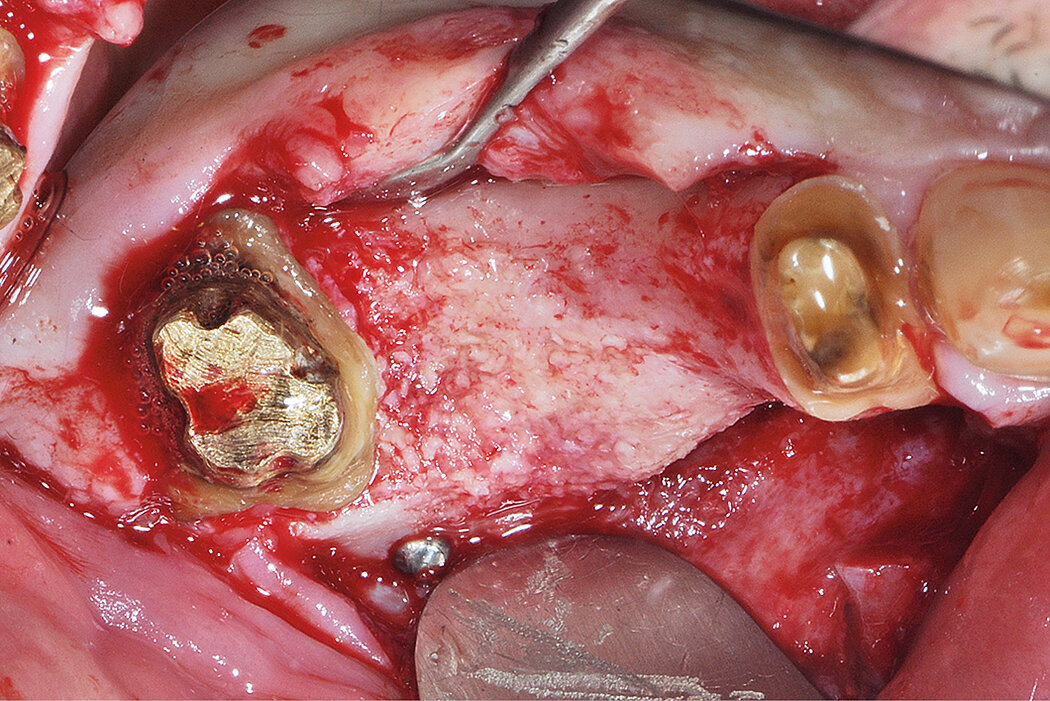
Conclusion
This approach was able to regenerate both the sinus and ridge bone deficiency in one surgery.